The BioArtificial Liver2
人工肝
混合型生物人工肝有效的血浆 净化技术与生物反应器结合
混合型/杂交型 (HBAL) 偏重于解毒作用的 ALSS 方式
hybrid bioartficial liver
血浆分离器、活性碳灌流器 肝细胞生物反应器
偏重于生物合成转化功能的 BLSS
H S Z- 2 0 0 0
肝 细 胞 反 应 器
聚丙烯腈膜—氮性肝性脑
水溶性血氨、尿素、胆红素
聚砜膜—致昏迷物质
脂溶性短链脂肪酸、硫醇、 酚
肝透析(liver dialysis)
腹水型:腹水、胸水及浮肿为突出表现
混合型:兼有肝性脑病和腹水表现
重肝的治疗进展
内科治疗
综合治疗 促肝细胞生长素 (HGF) 前列腺素 E1(PGE1 疗法) 抗病毒治疗
人工肝支持治疗
肝移植
高胆红素血症
危害
细胞变性坏死 细胞免疫性损伤 肾小管坏死“黄疸肾”
肝特异性解毒功能
参与糖、蛋白质、脂肪代谢
完成中间代谢,消除毒性物质、中间代谢产物 生物合成转化 分泌肝细胞生长因子等活性物质
灌 充 与 贴 壁
中 空 纤 维 内 腔 猪 肝 细 胞 的
VitaGen ELAD? 体外的肝帮助装置
VitaGen C3A 单元
肝母细胞瘤分离的消息灵通的 G2 细胞株 具有肝细胞代谢解毒功能 消息灵通的 G2 衍化出 C3A 细胞株 具有良好的肝细胞特异性功能
非生物型人工肝—血液 净化技术
血液透析
血液滤过
血浆灌流 血浆置换
非生物型人工肝—血液净化 技术
人工肝治疗的进展
肝移植
编辑版ppt
14
❖ 目前肝衰竭的内科治疗尚缺乏特效药物和手 段。肝移植因为价格昂贵、供肝短缺、文化 观念及技术因素的限制,还远未普及。所以 人工肝治疗在肝衰竭治疗中有重要的意义。
编辑版ppt
15
临床意义
遏制病程发展,促进肝脏自发恢复
• 重肝病人短期内发生大块肝细胞坏死
• 迅速出现黄疸,出血,昏迷,感染并发症
障碍、肝性脑病和腹水等为主要表现的一种临床综合征。
中编华辑医版学p会pt 感染病分会、肝病分会肝功能衰竭与人工肝学组10. 肝功能衰竭诊疗指南. 中华传染病杂志.2006,24:422
❖ 极度乏力,消化道症状,腹胀或腹水
❖ 黄疸进行性加深(TB>171umol/L或每天上升 17umol/L);
❖ 明显出血倾向,PTA<40%;
编辑版ppt
12
肝衰竭的治疗
❖ 既往最主要的是内科综合治疗。绝对卧床休息,所 以卧床休息可以保证肝脏的血液供应,有利于肝脏 的修复。
❖ 保肝降酶退黄,适当补充白蛋白或新鲜血浆,补充 凝血因子,酌情使用促肝细胞生长素;纠正水电解 质紊乱和酸碱平衡失调,重点在于防治并发症。
编辑版ppt
13
内科治疗
人工肝支持治疗
• 凶险、预后差,死亡率高,70~80%
• 人工肝:
❖ 迅速改善机体内环境 ❖ 部分解除和缓解毒性物质对肝脏全身毒害 ❖ 促进病情稳定 ❖ 为肝细胞再生创造时间
编辑版ppt
16
部分代偿衰竭肝脏的基本功能
• 功能:
合成功能(蛋白,凝血因子,胆固醇等) 转化解毒功能
• 免疫功能低下,导致感染 • 毒性物质↗ • 自由基、炎性细胞因子↗ • 引起肝性昏迷,水肿
选修人工肝和人工心脏
简称为 ALSS)。
人工肝脏是借助体外机械、化学或生 物性装置,暂时部分替代肝脏功能,从 而协助治疗肝脏功能不全或相关疾病的 方法。
人工肝脏能担负起暂时辅助或代替严 重病变的肝脏的功能,清除各种毒性物 质,代偿肝脏的代谢功能,直至自体肝 脏恢复或等待肝脏移植。
• * Immunity
肝功能衰竭
如果肝脏受到损害,往往会引起肝功能衰 竭。肝功能衰竭是指由于肝实质细胞(简 称肝细胞)功能障碍而引起的一种综合症, 包括黄疸、低蛋白血症、高氨血症、出血、 肾功能不全、代谢紊乱以至昏迷等临床表 现。
由于肝功能衰竭患者的大部分肝细胞 发生变性坏死,肝脏解毒、分泌、合成及 转化等功能受到严重影响,以致毒性物质 累积。
Glyconeogenesis and glycogenolysis • * Fat and Lipid Metabolism • * Synthesis of lipoproteins and cholesterol • * Protein Metabolism • * Synthesis of Plasma Proteins - albumin,
post-
Pre-therapy therapy
t
p
122.8± ALT (IU/L) 115.5 70.8± 86.8 2.04
<0.05
147.7±
AST (IU/L) 106.6
TB
488.3±
95.3± 81.6 300.6±
2.214
<0.05
(mol/L) DB (mol/L)
189.9 244.4± 100.0
人工肝治疗的进展
❖ 改善肝移植患者术前条件,顺利过渡术 中的无肝期以及术后肝脏无功能期
❖ 及时给予人工肝辅助治疗,显著提高治 愈率,缩短住院时间,节省医疗费用
人工肝治疗原理
借助 体外
循环 装置
血浆置换 血浆吸附 血液滤过 血液透析 生物装置
清除各种有害物质 暂时替代 补充蛋白质和凝血因子 肝脏功能
维持内环境稳定
急性肝衰竭 急性起病,2周以内出现肝衰竭的 临床表现
亚急性肝衰竭 起病较急,15日~24周出现肝衰竭 的临床表现
慢加急性肝衰 在慢性肝病基础上出现急性、亚急
竭
性肝衰竭临床表现
慢性肝衰竭 在慢性肝病基础上,出现肝功能进行 性减退或失代偿
肝衰竭的治疗
❖ 既往最主要的是内科综合治疗。绝对卧床休息,所 以卧床休息可以保证肝脏的血液供应,有利于肝脏 的修复。
性膜制成的滤过器时,加负
血 液
SMW-S
对流
压泵造成的跨膜压使血液中
的水分和溶质以对流的方式
MMW-S
滤过,等量的替代液被补充.
清除物质:
PB-S
滤 过
液
➢细胞因子(IL-6, IL-1, TNF)
➢中分子物质
血液灌流
Hemoperfusion(H
P)
补
原理:将血液送入血液灌流器,
液
与活性炭或树脂等充分接触,
❖ 保肝降酶退黄,适当补充白蛋白或新鲜血浆,补充 凝血因子,酌情使用促肝细胞生长素;纠正水电解 质紊乱和酸碱平衡失调,重点在于防治并发症。
内科治疗 人工肝支持治疗
肝移植
❖ 目前肝衰竭的内科治疗尚缺乏特效药物和手 段。肝移植因为价格昂贵、供肝短缺、文化 观念及技术因素的限制,还远未普及。所以 人工肝治疗在肝衰竭治疗中有重要的意义。
肝衰竭的护理体会
肝衰竭的护理体会肝衰竭是功能发生严重障碍或失代偿,出现以凝血机制障碍和黄疸、肝性脑病、腹水等为主要表现的临床症候群。
一般是由甲型肝炎病毒、乙型肝炎病毒或混合感染引起的消化道传染病。
病情重、进展快、预后差,病死率高,而且迄今尚无特效治疗,主要是对症支持治疗为主,必要时可行人工肝血浆置换,精心的护理对于患者治疗及抢救至关重要。
1 护理1.1饮食的护理患者有腹胀、腹泻、纳差、恶心、呕吐及厌油等消化道症状,应合理安排饮食,饮食以易消化,高维生素、低脂、高蛋白质的食物,少量多餐,减少机体代谢消耗,促进肝细胞再生。
合并上消化道出血时,应暂时禁食;合并肝肾综合征,低盐饮食,并尽量减少患者液体的摄入;合并肝性脑病,低蛋白饮食,在恢复期指导患者忌烟、酒及刺激性食物。
肝昏迷先兆者,低蛋白饮食,忌肉类食物。
1.2生命体征的监测生命体征是机体生命活动及重要脏器功能活动的客观反映。
因患者病情重,常合并上消化道出血、休克、多器官功能障碍等,护理工作中应该严密监测其生命体征,及时发现并发症,为早期诊断和治疗赢得宝贵的时间。
患者体温升高、心率变快或一般情况变差,是患者感染的迹象,应及时告知医师,配合医师予抗感染及降温等护理措施。
出现神志障碍,行为异常,可能是肝性脑病的发生,应及时做出相应处理。
血压降低是上消化道出血或感染性休克等严重并发症出现的征兆,予立即止血、输血等治疗措施迅速处理,并做出调整护理措施。
1.3基础护理加强基础护理,保持皮肤清洁干燥,皮肤瘙痒者给予温水擦浴,瘙痒严重时可涂止痒剂,严防抓伤而引起皮肤感染。
由于凝血酶原活动度降低故出现淤斑、淤点,注射部位淤紫或渗血,应在注射完毕后按压15~20min防止出血。
患者抵抗力低,细菌、真菌易在口腔内繁殖,引起口腔炎症,因此要保持口腔卫生,口腔护理1~2次/d,呕吐后给予温水漱口,餐后给予温水漱口,能下床时可刷牙1~2次/d,注意使用软毛刷,不要太用力。
1.4对黄疸的护理黄疸是由血清胆红素水平升高致使皮肤、粘膜、尿液颜色变黄。
人工肝治疗慢加急性肝功能衰竭,有效改善凝血功能、肝功能和炎症指标
【DX-10】人工肝治疗慢加急性肝功能衰竭,有效改善凝血功能、肝功能和炎症指标导读肝衰竭(Liverfailure)是多种因素引起的严重肝脏损害,导致其合成、解毒、排泄和生物转化等功能发生严重障碍或失代偿,出现以凝血功能障碍、黄疸、肝性脑病、腹水等为主要表现的一组临床症候群。
我国目前临床上以慢加急性肝衰竭为主,疾病进展快,病死率较高。
非生物型人工肝(Non-bioartificialliver,NBAL)已在临床广泛应用并被证明确有一定疗效。
本研究对在内科综合治疗基础上联合人工肝治疗的住院患者进行分析,评价不同人工肝治疗HBV相关慢加急性肝衰竭疗效,结论如下。
资料和方法1、一般资料:选择2014年1月至2017年12月在云南省保山市人民医院住院的HBV相关性慢加急性肝衰竭患者126例为研究对象,随机分为非人工肝组(对照组)和人工肝组(治疗组)。
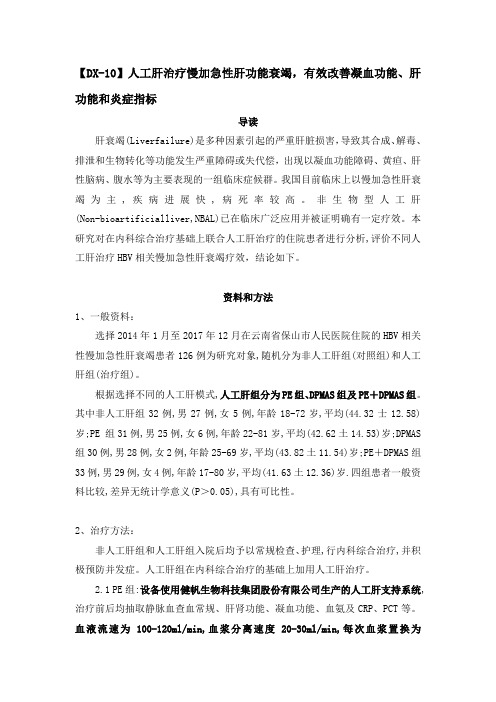
根据选择不同的人工肝模式,人工肝组分为PE组、DPMAS组及PE+DPMAS组。
其中非人工肝组32例,男27例,女5例,年龄18-72岁,平均(44.32士12.58)岁;PE 组31例,男25例,女6例,年龄22-81岁,平均(42.62土14.53)岁;DPMAS 组30例,男28例,女2例,年龄25-69岁,平均(43.82土11.54)岁;PE+DPMAS组33例,男29例,女4例,年龄17-80岁,平均(41.63土12.36)岁.四组患者一般资料比较,差异无统计学意义(P>0.05),具有可比性。
2、治疗方法:非人工肝组和人工肝组入院后均予以常规检查、护理,行内科综合治疗,并积极预防并发症。
人工肝组在内科综合治疗的基础上加用人工肝治疗。
2.1 PE组:设备使用健帆生物科技集团股份有限公司生产的人工肝支持系统,治疗前后均抽取静脉血查血常规、肝肾功能、凝血功能、血氨及CRP、PCT等。
血液流速为100-120ml/min,血浆分离速度20-30ml/min,每次血浆置换为2500-3500ml新鲜冰冻血浆+人血白蛋白10g,治疗时间约3h,治疗间隔时间2-4d,31例患者共行PE治疗73次,平均2.3次/例。
人工肝治疗的临床实践与研究进展
人工肝治疗的临床实践与研究进展韩涛,张倩南开大学人民医院,天津市人民医院消化(肝病)科,天津 300121通信作者:韩涛,****************(ORCID: 0000-0003-4216-6968)摘要:人工肝支持系统是治疗肝衰竭的重要方法之一,近年来非生物型人工肝在肝衰竭救治中的作用越来越受到认可,在非肝衰竭疾病中的应用也日益广泛。
临床上需要综合多种因素,合理选择非生物型人工肝治疗的时机及模式,规范化、个体化、精准化治疗及不同模式的优化组合是人工肝临床应用的趋势。
生物型人工肝有关种子细胞来源、生物反应器等关键技术不断完善,且部分已经进入临床试验阶段。
尽管人工肝治疗的临床实践与研究已取得很大进展,但仍面临不少挑战。
如何通过技术创新与优化组合进一步提高其疗效与安全性,如何通过高质量的临床试验获得更高级别循证医学证据,仍是目前亟需解决的难题。
关键词:肝,人工;肝功能衰竭;治疗学Clinical practice and research advances in artificial liver support therapyHAN Tao,ZHANG Qian.(Department of Gastroenterology and Hepatology,Tianjin People’s Hospital,Tianjin Union Medical Center Affiliated to Nankai University, Tianjin 300121, China)Corresponding author: HAN Tao,****************(ORCID: 0000-0003-4216-6968)Abstract:Artificial liver support system is one of the important therapies for liver failure, and in recent years, the role of non-bioartificial liver support system in the treatment of liver failure has been gradually recognized, with wide application in non-liver failure diseases. In clinical practice,various factors should be considered to reasonably select the timing and mode of non-bioartificial liver support therapy,and standardized,individualized,and precise treatment and optimal combination of different modes are the trend of the clinical application of artificial liver support therapy. There have been constant improvements in the key techniques of bioartificial liver support system such as seed cell source and bioreactor, and some of them have entered the stage of clinical trial. Although remarkable progress has been made in the clinical practice and research of artificial liver support therapy,there are still many challenges,and it is urgently needed to solve the problems of how to further improve its efficacy and safety through technological innovation and combination optimization and how to obtain higher-level evidence-based medical evidence through high-quality clinical trials.Key words:Liver, Artificial; Liver Failure; Therapeutics肝衰竭是临床常见的因肝功能严重损伤引起的危重症,尤其是急性(亚急性)肝衰竭和慢加急性肝衰竭,病情进展快,病死率高。
组合型人工肝的研究进展
组合型人工肝的研究进展黄玥,彭虹,罗新华贵州省人民医院感染科,贵阳 550000通信作者:罗新华,*********************(ORCID: 0000-0001-8285-3063)摘要:目前体外人工肝支持系统在各种原因导致的肝衰竭、肝移植前后无功能时期、严重胆汁性淤积等疾病中取得良好治疗效果。
其中非生物型人工肝(NBAL)通过各种模式互补组合广泛应用于临床,主要以改善机体凝血因子和白蛋白等物质的血浆置换模式联合其余增强清除体内有毒物质谱的模式。
以肝细胞的合成、转化功能为设计理念的生物型人工肝(BAL)近年也取得飞速发展。
肝衰竭患者先经NBAL解毒后,再予以BAL合成、转化体内活性物质,能更接近人体肝脏正常生理功能。
根据患者病情个体化组合NBAL模式,再结合疗效稳定的BAL是未来重症肝病患者体外支持治疗方向。
关键词:组合型非生物人工肝;组合型生物人工肝;治疗学基金项目:贵州省科学技术基金(黔科合基础-ZK[2021]重点013)Research advances in combined artificial liverHUANG Yue,PENG Hong,LUO Xinhua.(Department of Infectious Diseases,Guizhou Provincial People’s Hospital,Guizhou 550000, China)Corresponding author: LUO Xinhua,*********************(ORCID: 0000-0001-8285-3063)Abstract:At present,in vitro artificial liver support system has achieved a good therapeutic effect in the diseases such as liver failure due to various causes, non-function state before and after liver transplantation, and severe cholestasis. Non-bioartificial liver (NBAL)is widely used in clinical practice through various combinations of modes,mainly the plasma exchange mode for improving coagulation factors and albumin combined with other modes for enhancing the elimination of toxic substances in the body. Bioartificial liver (BAL),based on the design concept of the synthesis and transformation of hepatocytes,has achieved rapid development in recent years. Patients with liver failure can almost obtain the normal physiological function of human liver after NBAL detoxification and BAL synthesis and transformation of active substances in the body. NBAL mode combined with BAL with a stable therapeutic effect according to the conditions of the patient is the direction of in vitro support treatment for patients with severe liver disease in the future.Key words:Combined Non-biological Artificial Liver; Combined Bioartificial Liver; TherapeuticsResearch funding:Guizhou Science and Technology Foundation (ZK[2021] Key 013)肝脏是体内代谢功能最旺盛器官之一,对维持机体内环境平衡至关重要。
血液净化相关术语的英文缩略语
血液净化相关术语的英文缩略语1. APACHE‐Ⅱ acute physiology and chronic health evaluation‐Ⅱ 急性生理学和慢性健康评价Ⅱ2. PTT activated partial thromboplastin time 活化部分凝血酶原时间3. BAL(bioartificial liver,生物人工肝)4. CHD(continuous hem dialysis,持续血液透析)5. DFPP(double filtration plasmapheresis,双重膜血浆净化)6. FENa(excreted fraction of filtered sodium,滤过钠排泄分数)7. GCAP(granulocytapheresis,粒细胞净化疗法)8. LCAP(lymphocytapheresis,淋巴细胞净化疗法)9. PES(polyethersulfone,聚醚砜)10. PP(plasma perfusion,血浆灌流)11. PS(polysulfide,聚砜)12. QB(blood flow rate,血液流速)13. QD (dial sate flow rate,透析液流速率)14. TMP(Tran membrane pressure,跨膜压)15. UFR(ultra filtration rate,超滤过率)16. ARDS(acute respiratory distress syndrome,急性呼吸窘迫综合征)17. BUN(blood urea nitrogen,血尿素氮)18. CA(cellulose acetate,醋酸纤维素)19. CAVH(continuous arterio‐venous hemofiltration,持续动脉‐静脉血液滤过)20. CCr(creatinine clearance,肌酐清除率)21. CDA(cellulose diacetate,二醋酸纤维素)22. CHDF(continuous hemodiafiltration,持续血液透析滤过)23. CHF(continuous hemofiltration,持续血液滤过)24. CRRT(continuous renal replacement therapy,持续肾脏替代治疗)25. CTA(cellulose triacetate,三醋酸纤维素)26. CVVH(continuous veno‐venous hemofiltration,持续静脉‐静脉血液滤过)27. DHP(direct hemoperfusion,直接血液灌流)28. ECUM(extracorporeal ultrafiltration method,体外超滤过法)29. EOG ethylene oxide gas(环氧乙烷气)30. EVAL ethylene vinylalcohol(次乙基聚乙烯醇)31. GCS(Glasgow Coma Scale,Glasgow昏迷分级)32. HA(hemoadsorption,血液吸附)33. HMG‐1(high mobility group‐1,高移动性1组蛋白)34. HPM(high performance membrane,高性能膜)35. HPT(hepaplastintest,肝凝血活酶试验)36. HVH(high volume hemofiltrition,高容量血液滤过)37. IFN(interferon,干扰素)38. IRRT(intermittent renal replacement therapy,间歇肾脏辅助治疗)39. LDL(low density lipoprotein,低密度脂蛋白)40. NM(nafamostat mesilate,甲磺酸奈莫司他)41. PA(polyamide,聚酰胺)42. PAN(polyacrylonitri,聚丙烯腈)43. PEPA(polyester‐polymer alloy,聚酯‐多聚体合塑体)44. PMMA(polymethylmethacrylate,聚甲基异丁烯酸酯)45. PMX(polymyxin B immobilized fiber,多黏菌素固定化纤维)46. PS(polysufone,聚砜)47. PVP(polyvinyl pyrrolidone,聚乙烯吡咯酮)48. QF(filtration flow rate,滤液流量)49. SIRS(systemic inflammatory response syndrome,全身性炎症反应综合征)50. TNF(tumor necrosis factor,肿瘤坏死因子)51. β2‐m(β2‐microglobulin,β2‐微球蛋白)。
非生物型人工肝技术的优化与生物型人工肝研究进展
非生物型人工肝技术的优化与生物型人工肝研究进展周莉,杨颜榕,陈煜首都医科大学附属北京佑安医院肝病中心四科(疑难肝病及人工肝中心),肝衰竭与人工肝治疗研究北京市重点实验室,北京 100069通信作者:陈煜,**********************.cn(ORICD: 0000-0003-1906-7486)摘要:肝衰竭是临床常见综合征,进展快速,预后不良。
目前其内科治疗方法仍有限,人工肝治疗是一种有效的治疗方法。
非生物型人工肝技术在临床上广泛应用,其具体的启动时机、模式的选择、参数的设置需要临床医生根据疾病的病理生理机制及动态演变过程,结合患者具体情况决定。
与非生物型人工肝相比,生物型人工肝能更好地模拟肝细胞的生物学功能,目前其核心技术已取得实质性的进展,相关临床研究也在积极进行,在未来有广阔的发展前景。
本文就非生物型人工肝技术的优化及生物型人工肝相关进展进行总结与探讨,以期为人工肝技术的临床应用与研究提供参考。
关键词:肝,人工;肝功能衰竭;治疗学基金项目:国家重点研发计划项目(2022YFC2304400);北京市医院管理中心“登峰”人才培养计划(DFL20221501);高层次公共卫生技术人才培养计划(2022-2-012);北京市科技新星计划(20220484201)Optimization of non-bioartificial liver technology and research advances in biological artificial liverZHOU Li, YANG Yanrong, CHEN Yu.(Beijing Municipal Key Laboratory of Liver Failure and Artificial Liver Treatment Research,Forth Department of Liver Disease Center/Difficult and Complicated Liver Diseases and Artificial Liver Center,Beijing YouAn Hospital, Capital Medial University, Beijing 100069, China)Corresponding author: CHEN Yu,**********************.cn(ORICD: 0000-0003-1906-7486)Abstract:Liver failure is a common clinical syndrome with rapid progression and poor prognosis. Currently, there are still limited internal medical treatment methods for liver failure,and artificial liver support therapy is an effective treatment method. Non-bioartificial liver technology is widely used in clinical practice,and clinicians should determine the starting time,mode,and specific parameters of treatment according to the pathophysiological mechanism and dynamic evolution process of the disease, as well as the specific conditions of patients. Compared with non-bioartificial liver, biological artificial liver can better simulate the biological function of liver cells. At present, substantial progress has been made in its core technology, and related clinical studies are being conducted actively,suggesting a vast potential for future development. This article summarizes and discusses the optimization of non-bioartificial liver technology and the advances in biological artificial liver, in order to provide a reference for the clinical application and research of artificial liver technology.Key words:Liver, Artificial; Liver Failure; TherapeuticsResearch funding:National Key Research and Development Program of China (2022YFC2304400); Beijing Hospitals Authority’s Ascent Plan (DFL20221501);Construction Project of High-level Technology Talents in Public Health (2022-2-012);Beijing Nova Program (20220484201)肝衰竭是一种临床常见的综合征,以多种因素引起严重的肝功能损伤为特征,以黄疸、凝血功能障碍、肝肾综合征、肝性脑病、腹水为主要临床表现,病死率极高[1],肝移植是其唯一的治愈方法。
人工肝脏在急诊医学中的应用
人工肝脏在急诊医学中的应用关键词:暴发性肝衰竭(FHF) 人工肝在临床医学上,暴发性肝衰竭(fulminant hepatic failure,FHF)十分常见,休克肝、急性严重肝外伤、中毒性肝损害、多器官功能障碍综合征(multiple organ dysfunction syndrome,MODS)、急性胰腺炎伴肝功能严重损害、代谢性疾病等均可引起FHF。
由于此类患者的大部分肝细胞发生变性坏死、功能衰竭造成严重的代谢紊乱及毒性物质累积,反过来又影响肝细胞再生,形成恶性循环,依靠现有的病因疗法,一般对症支持疗法和动物源性促肝细胞生长因子,都不能代偿肝细胞功能,因而病死率极高,其救治是临床上亟待解决的问题。
众所周知,肝组织本身具有极强的再生能力,临床上对各种原因所致肝衰竭难以救治的原因,关键在于患者肝细胞发生大块或亚大块坏死,其坏死程度和速度远大于残存肝细胞的再生能力,再加上内毒素等综合因素作用,使坏死肝组织来不及再生、修复而致患者死亡。
在急诊医学范围内,严重休克病人较为常见,休克后易发展成FHF或MODS。
严重肝外伤合并胸部或毗邻器官的损伤往往也会造成严重的FHF,腹部伤而发生休克肝时,也常导致FHF。
FHF同时是肝胆外科的严重并发症之一,虽发生率不高但病死率极高。
FHF主要在手术后即出现,常在发病后1~2天内死亡。
FHF也是急性胰腺炎的常见并发症之一,且与胰腺疾患严重程度成正比,并可能成为急性胰腺炎患者死亡的主要原因。
如果患者在入院时肝功能有严重损害,预后往往不良。
药物及某些毒物也可引起FHF,如乙醇、氟烷、四氯化碳中毒、砷剂、有机磷、单胺氧化酶抑制剂、抗结核药物、扑热息痛、河豚鱼毒素、蜂毒、蛇毒、蝎毒、毒蕈中毒等。
MODS在急诊医学中较为常见,FHF在MODS中常常出现较早〔1〕。
由于肝脏受损,其代谢和解毒功能障碍,更促使MODS的发展。
目前国外学者认为,对于FHF最有效的疗法是肝移植〔2,3〕,但由于肝移植供体来源困难,而且手术复杂,费用较高,并须接受免疫抑制疗法等局限性条件,故不少学者长期致力于人工肝的研究,并将人工肝支持系统作为等待肝移植的过渡支持手段和替代疗法〔4~7〕。
3D培养体系下人来源诱导性多能干细胞向肝细胞的转化

3D培养体系下人来源诱导性多能干细胞向肝细胞的转化李嘉晋;王荣丽;李婷婷;何东;石伟【摘要】背景:生物型人工肝的构建有望成为治疗急性肝衰竭的有效方法,但构建人工肝的种子细胞来源、培养模式、营养获取等方面仍存在较多难题,制约血液净化-人工肝的发展与临床应用.目的:探讨在不添加外源血清等异种来源物质的条件下将人诱导性多能干细胞诱导分化为肝细胞样细胞的可行性.方法:应用含Transwell小室的6孔板构建3D培养体系,外源添加丙戊酸和尼克酰胺对人诱导性多能干细胞进行诱导分化,并将分化的肝细胞样细胞与生物补片共培养.实验分为5组:人诱导性多能干细胞为A组、正常肝细胞为B组、不添加尼克酰胺诱导分化的肝细胞样细胞为C组、添加尼克酰胺诱导分化的肝细胞样细胞为D组、在生物外科补片上培养的肝细胞样细胞为E组.倒置相差显微镜下观察D组肝细胞样细胞的形态;免疫荧光检测D组细胞中肝细胞核因子4α和甲胎蛋白的表达;荧光实时定量PCR和Western blot检测A、B、C、D组细胞中甲胎蛋白与白蛋白的mRNA和蛋白表达;流式细胞术检测A、C、D组细胞的分化效率;免疫细胞化学检测B组和E组细胞中胆盐输出泵蛋白的表达;ELISA检测D组和E组上清液中乳酸脱氢酶活性、白蛋白和尿素氮含量.结果与结论:①D组细胞由梭形逐渐转变成多边形;②D组细胞中肝细胞核因子4α和甲胎蛋白呈阳性表达;③D组细胞中甲胎蛋白、白蛋白的基因和蛋白表达明显高于A组和C组(P < 0.01);④B组和E组细胞中胆盐输出泵蛋白呈明显阳性表达;⑤E组细胞乳酸脱氢酶活性、白蛋白和尿素氮的含量明显高于D 组(P < 0.01);⑥结果表明,外源添加小分子化合物的三维培养体系和生物外科补片联合应用有助于促进诱导性多能干细胞在体外诱导分化为功能性肝细胞样细胞.【期刊名称】《中国组织工程研究》【年(卷),期】2018(022)029【总页数】6页(P4681-4686)【关键词】诱导性多能干细胞;肝衰竭;人工肝;Transwell小室;三维培养体系;生物外科补片;尼克酰胺;丙戊酸;生物人工肝;干细胞【作者】李嘉晋;王荣丽;李婷婷;何东;石伟【作者单位】西南医科大学临床医学院,四川省泸州市 646000;绵阳市人民医院,重症医学科,四川省绵阳市 621000;西南医科大学临床医学院,四川省泸州市 646000;绵阳市人民医院,重症医学科,四川省绵阳市 621000;绵阳市人民医院,肾病内科,四川省绵阳市 621000;绵阳市人民医院,重症医学科,四川省绵阳市 621000【正文语种】中文【中图分类】R394.2文章快速阅读:文题释义:生物型人工肝的构建:将人工培养的有生物活性的肝细胞填充在生物反应器内,构建体外生物反应装置模拟正常人体肝脏,以代替受损肝脏发挥解毒、合成与代谢功能。
人工肝在肝衰竭中的应用进展
, , mortality rate. Artificial liver can eliminate toxic substances in the body supplement essential substances and create opportunities for hepa , , tocyte regeneration and liver function recovery and in addition it can also prolong the waiting time for liver transplantation and thus acts as , , a bridge to liver transplantation. However the wide application of artificial liver is facing many difficulties nowadays such as shortage of , , , , , blood sources difficulties in cell sources a lack of satisfactory effects and high costs and therefore artificial liver treatment needs innova , , tion and improvement. New non - bioartificial liver systems developed in recent years such as double plasma molecular absorption system , , , molecular absorbent recirculating system continuous albumin purification system and plasma diafiltration can help to achieve a good clini
《临床肝胆病杂志》2024年1~10期重点号选题及执行主编

临床肝胆病杂志第40卷第2期2024年2月J Clin Hepatol, Vol.40 No.2, Feb.2024trolled clinical trial of the DIALIVE liver dialysis device versus stan⁃dard of care in patients with acute-on-chronic liver failure[J]. J Hepatol, 2023, 79(1): 79-92. DOI: 10.1016/j.jhep.2023.03.013. [12]BALLESTER MP, ELSHABRAWI A, JALAN R. Extracorporeal liversupport and liver transplantation for acute-on-chronic liver failure [J]. Liver Int, 2023. DOI: 10.1111/liv.15647. [Online ahead of print] [13]NICOLAS CT, HICKEY RD, CHEN HS, et al. Concise review: Liver re⁃generative medicine: From hepatocyte transplantation to bioartificial livers and bioengineered grafts[J]. Stem Cells, 2017, 35(1): 42-50. DOI: 10.1002/stem.2500.[14]DUAN ZP, XIN SJ, ZHANG J, et al. Comparison of extracorporealcellular therapy (ELAD®) vs standard of care in a randomized con⁃trolled clinical trial in treating Chinese subjects with acute-on-chronic liver failure[J]. Hepat Med, 2018, 10: 139-152. DOI: 10.2147/HMER.S180246.[15]LI LJ, DU WB, ZHANG YM, et al. Evaluation of a bioartificial liverbased on a nonwoven fabric bioreactor with porcine hepatocytes in pigs[J]. J Hepatol, 2006, 44(2): 317-324. DOI: 10.1016/j.jhep.2005.08.006.[16]LI WJ, ZHU XJ, YUAN TJ, et al. An extracorporeal bioartificial liverembedded with 3D-layered human liver progenitor-like cells relieves acute liver failure in pigs[J]. Sci Transl Med, 2020, 12(551): eaba5146.DOI: 10.1126/scitranslmed.aba5146.[17]SHI XL, GAO YM, YAN YP, et al. Improved survival of porcine acuteliver failure by a bioartificial liver device implanted with induced hu⁃man functional hepatocytes[J]. Cell Res, 2016, 26(2): 206-216.DOI: 10.1038/cr.2016.6.[18]WANG Y, ZHENG Q, SUN Z, et al. Reversal of liver failure using a bio⁃artificial liver device implanted with clinical-grade human-induced he⁃patocytes[J]. Cell Stem Cell, 2023, 30(5): 617-631. DOI: 10.1016/j.stem.2023.03.013.[19]CHEN HS, JOO DJ, SHAHEEN M, et al. Randomized trial of spher⁃oid reservoir bioartificial liver in porcine model of posthepatectomy liver failure[J]. Hepatology, 2019, 69(1): 329-342. DOI: 10.1002/ hep.30184.[20]WENG J, HAN X, ZENG FH, et al. Fiber scaffold bioartificial livertherapy relieves acute liver failure and extrahepatic organ injury in pigs[J]. Theranostics, 2021, 11(16): 7620-7639. DOI: 10.7150/ thno.58515.[21]FENG L, WANG Y, FU Y, et al. A simple and efficient strategy forcell-based and cell-free-based therapies in acute liver failure: hUC⁃MSCs bioartificial liver [J]. Bioeng Transl Med, 2023, 8(5): e10552. DOI: 10.1002/btm2.10552.[22]WANG J, REN H, LIU Y, et al. Bioinspired artificial liver system withhiPSC-derived hepatocytes for acute liver failure treatment[J]. Adv Healthc Mater, 2021, 10(23): e2101580. DOI: 10.1002/adhm.20210 1580.收稿日期:2023-11-20;录用日期:2023-12-20本文编辑:葛俊引证本文:HAN T, ZHANG Q. Clinical practice and research advances in artificial liver support therapy[J]. J Clin Hepatol, 2024, 40(2): 225-228.韩涛, 张倩. 人工肝治疗的临床实践与研究进展[J]. 临床肝胆病杂志, 2024, 40(2): 225-228.·消息·《临床肝胆病杂志》2024年1~10期重点号选题及执行主编为使作者了解本刊的编辑出版计划,及时惠赐稿件,《临床肝胆病杂志》编委会确定了2024年1~10期“重点号”选题及各期执行主编:1期肝血管病诊疗新进展⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅诸葛宇征2期人工肝治疗的临床实践与研究进展⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅韩涛3期关注慢性HBV感染与代谢功能障碍⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅李婕4期丙型肝炎病毒感染的消除⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅陈红松5期特殊人群乙型肝炎再认识⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅窦晓光6期肝胆胰疾病病理诊断⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅滕晓东7期转移性肝癌治疗进展⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅陈进宏8期中草药相关肝损伤的基础与临床研究进展⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅刘成海9期肝细胞癌转化治疗⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅蔡建强10期脂肪肝中医药治疗进展⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅⋅李秀惠为本刊重点号的投稿请注明“***重点号投稿”字样。
生物型人工肝支持系统种子细胞的来源与应用

生物型人工肝支持系统种子细胞的来源与应用朱雪晶1,黄伟健1,2,鄢和新1,21 上海赛立维生物科技有限公司,上海 2012102 上海交通大学医学院附属仁济医院麻醉科,上海 200127通信作者:鄢和新,***************(ORCID:0000-0001-8390-650X)摘要:迄今为止,重症肝炎、肝衰竭尚无特效治疗方法,病死率高达70%,是国内外危重症中的治疗难点。
肝移植术是目前终末期肝病最有效的治疗方法,然而仅有1%~2%的患者能够获得器官移植机会。
生物型人工肝支持系统通过体外机械、理化以及生物装置,清除患者体内蓄积的各种有害物质,代偿肝脏代谢功能,补充必需物质,改善内环境,帮助患者恢复肝功能,度过危险期,亦为患者肝移植争取宝贵时间,因此被认为是治疗终末期肝病的重要方法之一。
生物型人工肝的核心要素是肝细胞,本综述总结了当前生物型人工肝主要的肝种子细胞来源、3D培养方法以及相应的生物反应器培养系统,期望逐步实现肝细胞体外规模化制备,从而获得足够数量和质量的肝细胞这一临床应用亟待解决的核心问题。
关键词:肝,人工;种子细胞;培养技术基金项目:国家自然科学基金(82270635);上海市2020年度“科技创新行动计划”生物医药科技支撑专项(20S31906600)Source and application of seed cells in bioartificial liver support systemZHU Xuejing1,HUANG Weijian1,2,YAN Hexin1,2.(1. Shanghai Celliver Biotechnology Co.,Ltd.,Shanghai 201210,China;2. Department of Anesthesiology and Critical Care Medicine,Renji Hospital,Shanghai Jiao Tong University School of Medicine,Shanghai 200127, China)Corresponding author: YAN Hexin,***************(ORCID: 0000-0001-8390-650X)Abstract:So far, there are still no specific treatment methods for severe hepatitis and liver failure, resulting in a mortality rate of over 70%, and they are the difficulties in the treatment of critical illness in China and globally. Liver transplantation is currently the most effective treatment method for end-stage liver disease,but only 1% —2% of patients can receive the opportunity for organ transplantation. The bioartificial liver support system utilizes external mechanical, physical, and biological devices to remove various harmful substances accumulated in the patient’s body,compensate for the metabolic functions of the liver,supplement necessary substances, improve internal environment, promote the recovery of liver function, help patients get through the critical period, and save time for liver transplantation, and therefore, it is considered one of the important methods for the treatment of end-stage liver disease. Since hepatocytes are the core element of bioartificial liver, this article summarizes the sources of liver seed cells, 3D culture methods, and corresponding bioreactor culture systems and hopes to gradually solve the core issue of large-scale in vitro preparation of hepatocytes to obtain hepatocytes with adequate quantity and quality, which urgently needs to be addressed in clinical application. Key words:Liver, Artificial; Cell Sources; Culture TechniquesResearch funding:National Natural Science Foundation of China (82270635);Shanghai 2020“Science and Technology Innovation Action Plan” Biomedical Science and Technology Support Project (20S31906600)肝衰竭是由多种原因引起的严重肝脏损伤,其病死率极高[1]。
肝昏迷患者经人工肝治疗后成功行跨血型肝移植1例报告

孙爽,等. 肝昏迷患者经人工肝治疗后成功行跨血型肝移植1例报告肝昏迷患者经人工肝治疗后成功行跨血型肝移植1例报告孙爽,刘金泉,冯帅,王淑贤,徐祥美,戴德淑,王建红,蔡金贞,许传屾青岛大学附属医院器官移植中心,山东青岛 266000通信作者:许传屾,*****************(ORCID:0009-0004-0770-6409)摘要:本文报告1例经过人工肝支持治疗并成功过渡到肝移植的肝昏迷患者,经过积极治疗后患者后期恢复较好。
并且对肝移植手术的时机进行了讨论。
关键词:肝移植;肝功能衰竭;肝,人工基金项目:山东省自然科学基金面上项目(ZR2023MH240);北京肝胆相照公益基金会“2023年度人工肝专项基金”(iGandanF-1082023-RGG037);青岛大学附属医院“临床医学+X”科研项目(QYFY+X202101060)Successful trans-blood liver transplantation after artificial liver support therapy in a patient with hepatic coma: A case reportSUN Shuang,LIU Jinquan,FENG Shuai,WANG Shuxian,XU Xiangmei,DAI Deshu,WANG Jianhong,CAI Jinzhen,XU Chuanshen.(Organ Transplantation Center, The Affiliated Hospital of Qingdao University, Qingdao, Shandong 266000, China)Corresponding author: XU Chuanshen,*****************(ORCID: 0009-0004-0770-6409)Abstract:This article reports a patient with hepatic coma who underwent artificial liver support therapy and liver transplantation successfully,and the patient recovered well in the later stage after active treatment. This article also discusses the timing of liver transplantation.Key words:Liver Transplantation; Liver Failure; Liver, ArtificialResearch funding:General Project of Shandong Natural Science Foundation (ZR2023MH240);The “2023 Artificial Liver Special Fund” of the Beijing Hepatobiliary Mutual Welfare Foundation (iGandanF-1082023-RGG037); The “Clinical Medicine+X” Research Project of Qingdao University Affiliated Hospital (QYFY+X202101060)肝衰竭是临床常见的严重肝病症候群,病情进展快,病死率极高。
中国人工肝研究——跟跑者迈向领跑者
『f1同 发明 与 专和j
China Invention& Patent
V_ ቤተ መጻሕፍቲ ባይዱ1.15 NO.4 Apr. 2018
中国人工肝研 究 跟跑 者迈 向领跑 者
李 娟‘。!
(1.传 染病 诊 治 国家重 点实 验窒 ,杭 州 3l0003: 2.感染 性疾 病 诊治 协 同创新 中心 ,杭 州 3l0003; 3.浙汀 大学 医学 院 第一 附属 医院 ,杭 州 3 l0003
. 37.
李 兰娟 :中 国人 工肝 研究— — 跟跑 者迈 向领 跑者
201 8年第 4期
1 国 内外 人 工肝 发展 史 1956年 ,Sorrention证 明 了新 鲜 肝 组 织 匀 浆 的 解
毒 能力 ,首 次提 出了 “人工 肝脏 ” 的概 念 。从 那 时至今 , 人 工 肝脏 经 历 了半 个多 世 纪 的 发展 过 程 。 回顾这 一 段 历 史 ,大 致 可 分为 以下 几 个 阶段 。 我 国人 工 肝 的研 究 也 由空 白开 始迎 头追 赶 ,从 跟跑 者 向领 跑者 迈 进 。 1.1 二 十世 纪 五六 十年代 —— 人 工肝 研究 的兴 起
作者简 介 :李 兰娟 (1947一 ),女 ,浙 江绍 兴人 ,感 染病 学专 家,浙江大学教授 、博士 生导 师,传 染病诊 治国 家重点 实验 室主任 ,感 染性疾病诊 治协 同创新 中心主任 ,全 国人 工肝培训基地 主任 ,树 兰医疗发起人 2005年 当选为中国工程 院院士 荣获 国家科学技 术进步 奖特等 奖、创新 团队奖、一 等奖和二 等奖等
凝血 因子等必需物喷
生物型 以体外培 养肝细 胞为基 础所构建的体外生物反应装置 ,主要有 Li—BAL系统、 具有I¨=脏特异性解毒
C3A细胞与L-02永生化肝细胞低温保存条件下的生物学特性比较

C3A细胞与L-02永生化肝细胞低温保存条件下的生物学特性比较李安全;李庆勇;张清华;蒋知新;沙杭;高德禄;高毅【摘要】背景:获得大量功能良好的肝细胞是生物人工肝的核心.探索出一种可靠的肝细胞低温保存方法进而构建一个肝细胞库是目前生物人工肝研究的热点.目的:比较用UW液在4 ℃条件下保存已经进入Ⅲ期临床试验的C3A细胞与国内构建的永生化肝细胞株L-02细胞的生物学特性.方法:贴壁培养C3A与L-02细胞,胰酶消化,制备成细胞悬液,UW液保存.4 ℃低温保存0,24,48及72 h后,采用流式细胞术分别测定细胞存活率与凋亡率,测定谷草转氨酶与乳酸脱氢酶释放、尿素合成功能及白蛋白分泌功能.结果与结论:随低温保存时间延长,C3A与L-02细胞存活率呈下降的趋势,但C3A细胞的存活率明显高于L-02细胞(P < 0.01);细胞凋亡率呈上升趋势,但48 h后C3A细胞同L-02细胞无差异(P > 0.05).谷草转氨酶及乳酸脱氢酶释放呈现上升的趋势,但C3A细胞明显低于L-02细胞(P < 0.01).白蛋白分泌功能呈下降的趋势,但C3A细胞明显优于L-02细胞(P < 0.01).尿素合成功能呈下降的趋势,但是L-02细胞明显优于C3A细胞(P < 0.01).结果提示,UW液4 ℃保存C3A细胞与L-02细胞时间不易超过48 h.以C3A细胞为材料的人工肝可能更适用于肝功能衰竭合并低白蛋白血症,以L-02细胞为材料的人工肝更适用于肝功能衰竭合并肝性脑病.%BACKGROUND: A large number of functional liver cells is the core of bioartificial liver. It is the existing research focus of bioartificial liver to explore a reliable method of cryopreservation of liver cells and to construct liver cell bank.OBJECTIVE: To compare the biological characteristics of C3A hepatocytes that has entered clinical Ⅲ stage test and L-02 immortalized hepatocytes stored in UW solution at4 ℃ .METHODS: The C3A hepatocytes and L-02 hepatocytes were adherent cultured, digested by 0.25% trypsinization, prepared into cell suspension, and stored in UW solution. At 0, 24, 48, 72 hours of hypothermic storage (4 ℃), the cell viability rate and cell apoptosis rate were measured using flow cytometry. Lactate dehydrogenase and aspartate aminotransferase release, the ability of hepatocytes to synthesize urea and secrete albumin were also determined.RESULTS : The cell viability of C3A hepatocytes and L-02 hepatocytes was degraded following the time, but the cell viability of C3A hepatocytes was higher than L-02 hepatocytes (P < 0.01). Cell apoptosis was increased, but there was no difference between C3A hepatocytes and L-02 hepatocytes after 48 hours (P > 0.05). The lactate dehydrogenase and aspartate aminotransferase release were ascended, but the release of C3A hepatocytes was lower than L-02 hepatocytes (P <0.01). The ability of hepatocytes to secrete albumin was decreased, but the ability of C3A hepatocytes was better than L-02 hepatocytes (P < 0.01). The ability of hepatocytes to synthesize urea was also decreased, however, the ability of L-02 hepatocytes was better than C3A hepatocytes (P < 0.01). Results demonstrated that, the time of the C3A hepatocytes and L-02 hepatocytes which are hypothermicaly stored (4 ℃ ) in UW solution should not exceed 48 hours. The artificial liver prepared by C3A hepatocytes is more suitable for the liver function failure combined low albuminaemia, and artificial liver prepared by L-02 hepatocytes fits the liver function failure combined hepatic encephalopathy.【期刊名称】《中国组织工程研究》【年(卷),期】2011(015)003【总页数】5页(P473-477)【关键词】生物人工肝;低温保存;永生化肝细胞;C3A细胞;L-02细胞【作者】李安全;李庆勇;张清华;蒋知新;沙杭;高德禄;高毅【作者单位】解放军第三○五医院,北京市,100017;解放军第三○五医院,北京市,100017;南方医科大学研究生院,广东省广州市,501515;解放军第三○五医院,北京市,100017;解放军第三○五医院,北京市,100017;解放军第三○五医院,北京市,100017;解放军第三○五医院,北京市,100017;南方医科大学珠江医院肝胆二科,广东省广州市,510253【正文语种】中文【中图分类】R3180 引言生物人工肝(bioartificial liver support system,BALSS)为肝功能衰竭的治疗开辟了新的途径[1]。
血浆置换疗法
血浆置换疗法血浆置换(plasma exchange,PE)属于血液净化技术的一部分就是将患者的血液抽出体外后,将血浆中的致病成分选择性地分离后弃去,然后将血浆的其他成分以及所补充的平衡液或白蛋白输回体内,以清除血浆内的致病物质的一种血液净化方法。
血浆置换又称血浆分离(plasmaphresis)。
“Plasmaphresis”是希腊语,意思是血浆清除(plasma removal)。
1914年Abel等最先提出血浆清除法,就是应用沉淀的方法将血浆和血细胞分离,弃去血浆后,再将血细胞和重新配置的白蛋白液输回体内。
直到20世纪60年代才出现封闭式的离心分离装置,70年代又发明了膜式血浆分离装置。
此后,膜式血浆置换方法得到了广泛的作用。
近年,又提出的血浆成分分离,其通过双重膜式滤过(double filtration)或冷滤过(cryofiltration)等方法将血浆的成分进行分离。
血浆置换可用于治疗200多种疾病,包括肾小球基底膜抗体肾炎、免疫复合物肾炎、坏死性血管炎肾损害、狼疮性肾炎、血液粘滞性过高综合征、重症肌无力、急性格林巴利综合征、肾移植排异反应等。
血浆置换治疗原理血浆置换主要是先分离出血浆,再从其中清除某些疾病的相关致病因子,这些因子包括自身免疫性疾病的抗体(IgG、IgM等)、沉积于组织的免疫复合物、异型抗原和异常增多的低密度脂蛋白和一些副蛋白,如冷凝球蛋白及游离的轻链和重链,有时还包括一些同蛋白结合的毒素。
由于血浆置换能直接和快速地清除一些直接导致疾病的因子,所以通过它的治疗常常收到意外的疗效,后者是用一些口服或静脉注射免疫抑制剂所不能达到的。
一般而言,抗体就是IgG,其分子量为150×103左右;而免疫复合物分子量多为100×103左右。
换言之,由于它们全部被包含在丢弃血浆之中,因此丢弃血浆(血浆置换)也就等于清除了致病因子。
血浆置换的作用机制还有非特异性的一面,这也是不可忽视的,例如在一些情况下,血浆置换的治疗作用不可能与减少了非特异性的炎性介质有关,如补体和纤维蛋白原,甚至它的一些疗效可能与尚不清楚因子的减少有关。
- 1、下载文档前请自行甄别文档内容的完整性,平台不提供额外的编辑、内容补充、找答案等附加服务。
- 2、"仅部分预览"的文档,不可在线预览部分如存在完整性等问题,可反馈申请退款(可完整预览的文档不适用该条件!)。
- 3、如文档侵犯您的权益,请联系客服反馈,我们会尽快为您处理(人工客服工作时间:9:00-18:30)。
Susana Candia Jahi Gist Hashim Mehter Priya Sateesha Roxanne Wadia
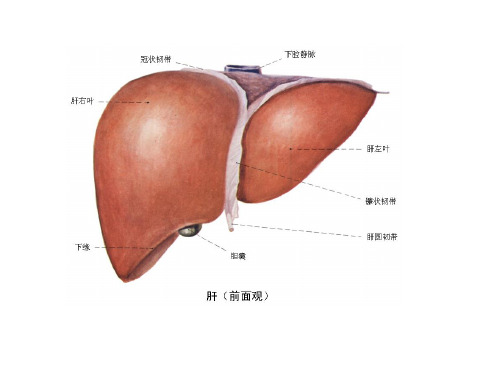
Biology of the Liver
Right lobe Gallbladder Inferior Vena Cava Left lobe Falciform Ligament
Liver Dialysis Unit
• FDA approved in 1994 • Plate dialyzer with blood on one side, dialysate is a mixture of sorbents, activated charcoal being the essential component. • For a substance to be removed, must be dialyzable and able to bind to charcoal. • “Bridge to recovery” for treat acute hepatic encephalopathy and overdoses of drugs • Post-market trials have shown the LDU to be effective in improving physiological and neurological status.
HepAssist 2000 System
• Four components: a hollow fiber bioreactor containing porcine hepatocytes, two charcoal filters, a membrane oxygenator, and a pump. • Must be used in conjunction with a commercially available plasma separation machine • Blood separated; plasma processed through charcoal filters to remove particulates, bacteria, then enters bioreactor • Hepatocytes must be heated and oxygenated • FDA mandated full Phase III trials
MARS®
• Limited to investigational use in US. • Hollow fiber membrane hemodialyzer. • Blood on one side, human albumin on other. • Albumin recycled through circuit containing another dialyzer and carbon and anion exchanger adsorption columns. • Removes both water-soluble and protein bound substances • Keep valuable proteins • Trial have found it safe and associated with clinical improvement
Kidneys
Abdominal Aorta
Graphic Courtesy of: /s-crina/liver-anatomy.htm
What does the Liver do?
Among the most important liver functions are: • Removing and excreting body wastes and hormones as well as drugs and other foreign substances • Synthesizing plasma proteins, including those necessary for blood clotting • Producing immune factors and removing bacteria, helping the body fight infection Other important but less immediate functions include: • Producing bile to aid in digestion • Excretion of bilirubin • Storing certain vitamins, minerals, and sugars • Processing nutrients absorbed from digestive tract
Works in Progress: Points to Consider
Bioreactor designs/Membrane configurations
Cellular vs. Acellular system Porcine vs. Human hepatocytes Point in Development
LIVERx2000
• Hollow fiber cartridge • Primary porcine hepatocytes suspended in a cold collagen solution and injected inside fibers • Blood circulates outside the hollow fibers • Designed to treat both acute and chronic liver failure • Phase I/II clinical trials are underway to test the safety of efficacy of this device • Anyone treated with the LIVERx2000 will be monitored for PERV
•Patients are in waiting list ranked according to severity of disease and life expectancy among other variables.
•Can be from a cadaveric donor or from a live donor.
BLSS
• Extracorporeal hemofiltration hollow fiber membrane bioreactor with 100 grams of primary porcine hepatocytes • Whole blood is filtered • Contains blood pump, heat exchanger, oxygenator to control oxygenation and pH, and hollow fiber bioreactor • Currently undergoing phase I/II clinical trials • Patients show some improvement
ELAD®
• Uses cultured human hepatocytes express normal liver-specific metabolic pathways. hollow fiber dialyzer. • Dialyzer cartridge connected to continuous hemodialysis machines, like those used for renal therapy. • Blood separated into a cellular component and a plasma component. • Plasma through dialyzer, hepatocytes on outside of hollow fibers. • Currently involved in a phase 2 clinical trial to evaluate the safety and efficiency.
•Involves heavy use of immunosuppressants during and after surgery.
•The risk of rejecion is always present.
Patients
What does a BioArtificial Liver need to do?
Enabling Technologies
• Hemodialysis/hemofiltration hollow fibers- controlled interaction of cells and circulating fluids • Maintenance and creation of a cell line • Immortalizing cells • Encapsulation-envelopment of hepatocytes in a polymeric matrix. • Microcarriers- polymeric particles containing cells
4)
5)
6) 7)
The synthetic component must be fully biocompatible, integrity of the material and parts must also be demonstrated The device must be able to introduce the therapeutic and regulatory molecules that a healthy liver provides, and it must also filter substances from the blood the way that the normal liver does. Must be immunocompatible. Blood must perfuse properly through system